
Plantar Fasciitis
Plantar fasciitis can be a very painful and long term condition for a lot of people and effective treatment often requires a good understanding of the structures and mechanisms involved, both from the patient and the treating practitioner.
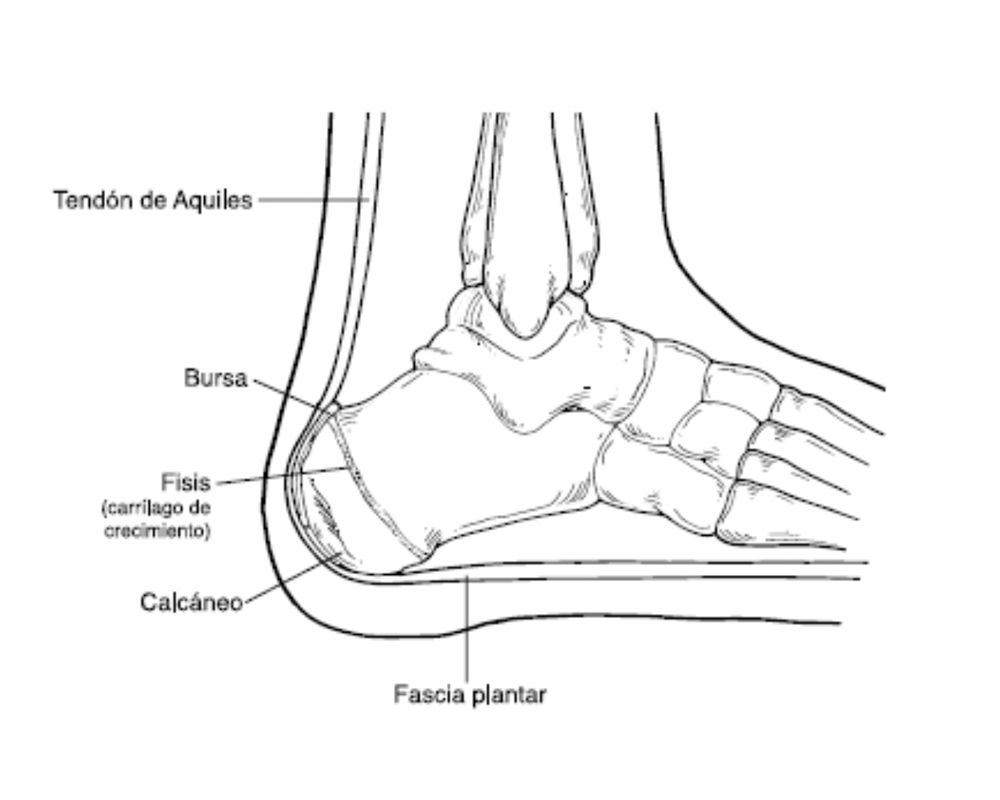
The plantar fascia is a piece of connective tissue (think leather, or the gristle in a steak) that runs from the heel of your foot to the arch.
The role of the plantar fascia is to collect energy through gait cycle, at heel strike, then stiffen the foot before toe off, by winding itself over the the head of the first metatarsal. It then releases it’s energy at toe off, where it’s structure becomes slack again. This mechanism is described as a “windlass” and is similar to the way an old fashion well works, when you wind a bucket up and down, rolling the rope over a wooden pole.

There multiple theories as to how the plantar fascia can become injured, including excessive foot pronation, excessive hip rotation as well as reduced hip rotation! Likely different degrees of all these factors will contribute differently to the injury in different individuals.
Most people with plantar experience pain have a long story to tell, and find many half successful treatments along the way. Pain is usually felt on the bottom of the foot in just in front of the heel and spreading forward towards the toes. It is often worst a few hours or the day after exercise, and can be excruciating first thing out of bed in the morning. Hard floors are reported as very aggravating, and soft sand walking can quickly overload it.
But plantar fasciitis is essentially a degenerative condition, and being degenerative will usually require initially gentle, then progressively greater loading and strengthening of the involved tissues to resolve. Loading too fast can be really aggravating, and complete rest will often just lead to further degeneration. The challenge for the therapist is to find the sweet spot for the patient in front of them.
Taping and bracing can help relieve symptoms in the short term, which can be really useful for sporting matches or workouts. Some subgroups of the population might also benefit from an orthotic to reduce pronation during stride.
Exercises for the foot hip and calf are a mainstay for long term resolution. And in particular the Rathlieff raise, incorporating active big toe flexion and a heel raise has been found to be just indispensable in our clinic.
The big toe is placed upon a towel or custom device as pictured. The patient pushes firmly down into the towel with the toe and then performs a heel raise as normal. Most people will need a little supervision during their exercises and a little customisation around their hip and knee movements. But we’ve found in clinic that the hardest part of this rehab programme is making the patient remember that they’ve got plantar fasciitis after the second week, and that they have to keep doing the movements for another week or two, to get rid of the problem. And this has been really welcome change for us, for a problem that used to have a lot of wish washy answers, and ongoing chronic pain.
Written by Michael O’Doherty, Head Chiro at Chiropractic Moves in Rosalie Village
Visit their website here: https://www.chiropracticmoves.com.au/










